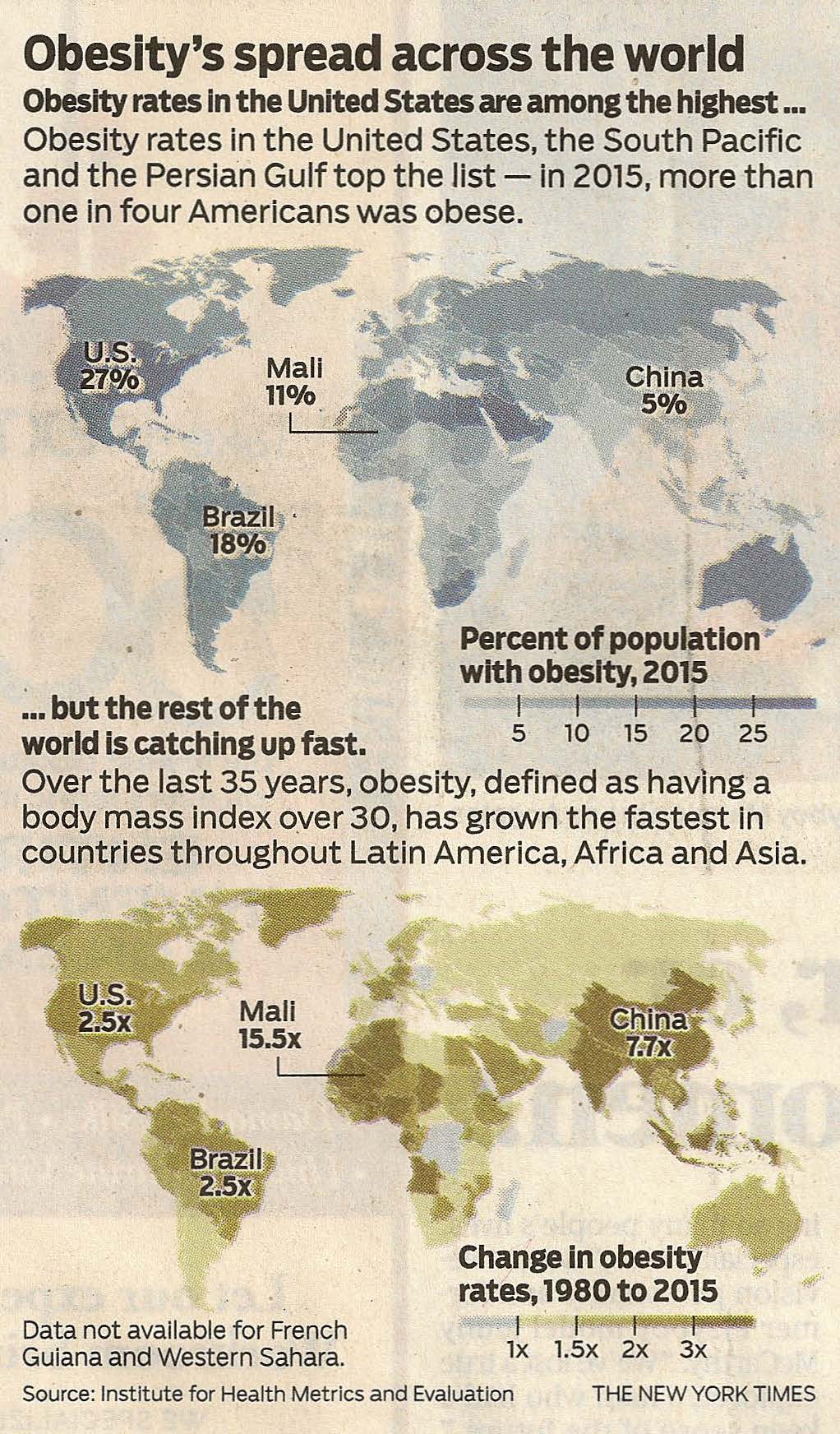
The CDC reports that 7 out of 10 Americans are overweight or obese and almost 4 out of 10 Americans are obese.
The CDC reports that 7 out of 10 Americans are overweight or obese and almost 4 out of 10 Americans are obese.
There is an underlying pattern of racial and ethnic disparity. Almost half of Hispanics and blacks are obese with obesity rates for 2015-2016 of 47% and 46.8% for adult Latinos and non-Hispanic blacks respectively.
Obesity is most readily defined by Body Mass Index (“BMI”) which takes a person’s weight in kilograms and divides it by their height in meters squared. For adults, those with a BMI between 18.5 and 24.9 are considered to have a normal weight. A BMI between 25 and 29.9 is considered overweight and anything above 30 is deemed obese. The NIH provides a calculator for you to determine your own BMI.
It is apparent to anyone following these statistics or even just walking down the street that current efforts to control the obesity problem have failed to reduce obesity rates.
We have learned that visceral fat or “belly” fat within the abdomen hijacks the metabolism by secreting the cytokine resistin. This cellular hormone antagonizes insulin, blocking sugar from entering cells or reaching the brain. It saps energy, shuts down the metabolism, causes brain fog, and hunger. Cellular hormones are secreted directly into the portal circulation and the body’s protein factory, the liver, is commandeered to produce bad lipids which cause strokes and heart attacks. Mesenteric fat thickness is closely correlated with carotid intimal narrowing. Belly fat doesn’t just shorten your life, it reduces its quality with sleep apnea, gastric reflux, type 2 Diabetes mellitus, heart attacks, strokes, autoimmune diseases, and cancers.
New technology facilitates a new approach to the problem. Rather than just starving this belly fat and letting it remain in place as do current bariatric surgical alternatives, removing it this visceral fat in a minimally invasive procedure may prove to be a simpler, more direct and permanent, safer and highly effective alternative. Endoscopic visceral lipectomy could be just be what the doctor ordered. It is clearly time to seek new approaches and fresh solutions as obesity rates continue to rise.

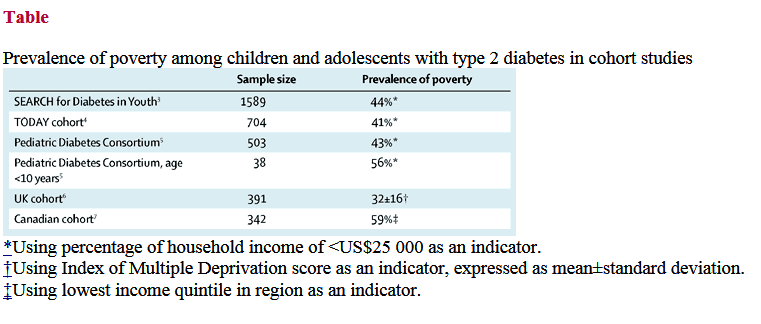 It is clear that the family must be involved in the treatment of the patient. But, it is only by recognizing, openly discussing and addressing the underlying conditions responsible for these financial, racial and ethnic disparities in our society that we can make meaningful incursion upon this growing scourge on the future of our youth.
It is clear that the family must be involved in the treatment of the patient. But, it is only by recognizing, openly discussing and addressing the underlying conditions responsible for these financial, racial and ethnic disparities in our society that we can make meaningful incursion upon this growing scourge on the future of our youth.